Key Takeaways for Cold Chain Readiness
Summary: A camp vaccination cold chain plan should move in sequence: define campaign assumptions, map every storage point and handoff, size transport and session capacity, monitor temperatures, and prepare contingencies before launch.
Cold chain planning is not a refrigerator shopping list.
In a camp campaign, the cold chain runs through people, roads, session timing, vaccine handling, documentation, and decision authority. A working refrigerator can still support a poor campaign if the mobile team opens carriers too often, if the queue stalls in full sun, or if no one knows who can quarantine stock after a suspected temperature excursion.
The safest plans start with the campaign design and work outward to equipment. Vaccine-specific rules should come from manufacturer labeling, national immunization policy, and practical guidance such as WHO’s Immunization in Practice guidance. Field teams should not invent handling rules because the road is bad or the session is crowded.

A useful cold chain question is not, “Do we have enough cold boxes?” It is, “Can the vaccine move from controlled storage to administration and back through a documented chain of decisions without guesswork?”
Cold chain readiness sequence
- Define the target group, vaccine presentation, session model, staffing pattern, and daily workload.
- Map central storage, camp storage, temporary holding areas, mobile carriers, vaccination tables, and return paths.
- Size capacity around vaccine volume, diluents when required, conditioned ice packs, reserve stock, and session duration.
- Assign staff to temperature monitoring, carrier discipline, documentation, and escalation.
- Prepare contingency actions for power failure, delayed transport, blocked roads, crowd-control delays, and suspected excursions.
Start With Campaign Assumptions Before Equipment Lists
The first cold chain meeting should not begin with equipment. It should begin with assumptions.
Who is the campaign trying to reach? Which vaccine presentation will be used? Are sessions fixed at the health post, pushed out through mobile teams, or split between both? How many tables will operate, who will record doses, and where will people wait before screening?
Those questions sound clinical, but they decide the logistics. A fixed-site campaign may lean on a camp health post refrigerator and carefully managed table carriers. An outreach team may depend on packout discipline, transport timing, and a return route that still protects unopened stock at the end of the day.
Unclear assumptions create familiar cold chain trouble: refrigerators filled with stock that never moves, carriers packed beyond safe handling space, or vaccines sitting outside controlled storage while teams debate where the next session will open.
Quick Tip: Sort planning assumptions into three columns: confirmed, pending, and high-risk. Confirmed items guide today’s equipment plan. Pending items need owners and deadlines. High-risk items deserve a fallback route, fallback storage point, or reduced session plan.
That simple sorting method lets logisticians and clinical leads revise the cold chain plan without tearing it apart. If an outreach point shifts because a road floods, the team changes the route, handoff, and packout assumptions tied to that site. The whole campaign map does not need to be rebuilt.
I have found that the most useful assumption sheet is blunt. It names what the team knows, what it is waiting on, and what could break the plan by sunrise.
Map Every Storage Point, Handoff, and Return Path
A camp cold chain map should follow the vaccine, not the organogram.
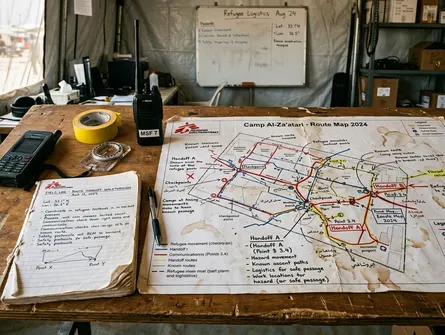
Start at the central store, then trace the movement to the camp health post, any temporary vaccine holding area, the mobile team carrier, the vaccination table, and the end-of-day return. Mark each stop where a container is opened, checked, signed over, parked, shaded, delayed, or returned.
Each handoff needs four things: a responsible role, a time window, a temperature check procedure, and a fallback contact. Without those details, a “handoff” is just a hope that two busy people meet at the right place.
In one route walk-through I joined, the paper map looked clean until we stood at the checkpoint where vehicles actually queued. The satellite route had missed the waiting area, the crowd-control barrier, and the fact that the only shade disappeared by late morning. That changed the carrier plan more than the road distance did.
Camp geography does not behave like a logistics diagram. Rough access roads slow vehicles. Security checkpoints interrupt timing. Flood-prone paths turn short walks into detours. Limited shaded waiting areas can extend exposure time because vaccination tables open carriers more often when the line becomes disorderly.
What to mark during the route walk-through
- Where vehicles park and whether carriers remain shaded during unloading.
- Where temperature checks happen and who records them.
- Where stock is held if a team arrives before the session site is ready.
- Where opened and unopened stock are separated at the end of the day.
- Who receives a call if transport, security clearance, or power fails.
Monitoring reports show that route problems usually appear at the edges: the parked vehicle, the waiting room, the return path, the crowded doorway. The map has to include those edges.
Size Cold Chain Capacity for Volume, Time, and Handling
Capacity planning is plain work. You compare what must stay cold with the real internal space of the equipment that will carry it.
That means vaccine vials, diluents if the product requires them, conditioned ice packs, dividers or foam pads specified by the equipment guidance, reserve stock, and the space needed to keep items from being crushed or badly arranged. The right answer comes from product dimensions, campaign microplans, national immunization tools, and actual equipment specifications. It should not come from a rough guess made beside a loaded vehicle.
Storage capacity and session capacity are not the same thing.
A refrigerator may hold stock safely overnight, but a vaccination team still needs usable carrier space at the table. A carrier packed tightly with too many vials can leave too little room for conditioned ice packs and stable handling. The result is not efficiency; it is a fragile session where every lid opening matters more than it should.
Note: Do not treat the listed size of a refrigerator or carrier as fully usable session capacity. Packaging, ice packs, airflow, vial arrangement, and the need to separate stock all reduce what the team can safely use.
Pre-Campaign Cold Chain Dry Run Checklist
- Verify usable carrier volume with empty cartons or nonclinical training materials.
- Confirm ice pack conditioning under the current camp temperature, not last season’s assumptions.
- Walk the physical transport route and identify where carriers may be opened.
- Practice the end-of-day return, including separation of opened, unopened, and quarantined stock.
- Check that every temperature log, equipment identifier, and escalation contact is available before vaccines move.
This is where a dry run earns its time. A team that packs training materials into real carriers, walks the route, sets up the table, and practices the return will find tight spots before the vaccine is at risk.
Control Temperature During Transport and Vaccination Sessions
Session-day temperature control starts before the first person reaches the queue.
Teams need to condition ice packs according to the equipment guidance, load carriers the same way each time, and assign one person to carrier discipline. That person does not need to outrank the clinical staff. They do need clear authority to say when the lid stays closed.
Shade is a cold chain control. So is table layout. So is the way the queue bends around the screening point.
If vaccinators have to reach across recorders to access vials, the carrier will be opened more often. If crowd managers push the line too close to the table, staff rush handling steps. If the waiting area has no shade, sessions may need to pause or reorganize, extending the time stock spends in field conditions.
Mixed clinical-logistics workflows need one shared rule for carrier access. Vaccinators, recorders, crowd managers, and logistics staff should know who may open a carrier, when checks are documented, and what happens when the table needs more stock.
Practical session controls
- Assign one named person to manage carrier opening and closing.
- Keep the active carrier shaded and stable, away from crowd pressure.
- Separate the working stock from reserve stock when the equipment plan allows it.
- Make temperature checks part of the session rhythm, not an afterthought at closing.
- Stop and escalate when a reading, container condition, or handling error falls outside the agreed rule.
The goal is not to make the session slow. The goal is to make safe handling ordinary enough that staff keep doing it when the line gets noisy.
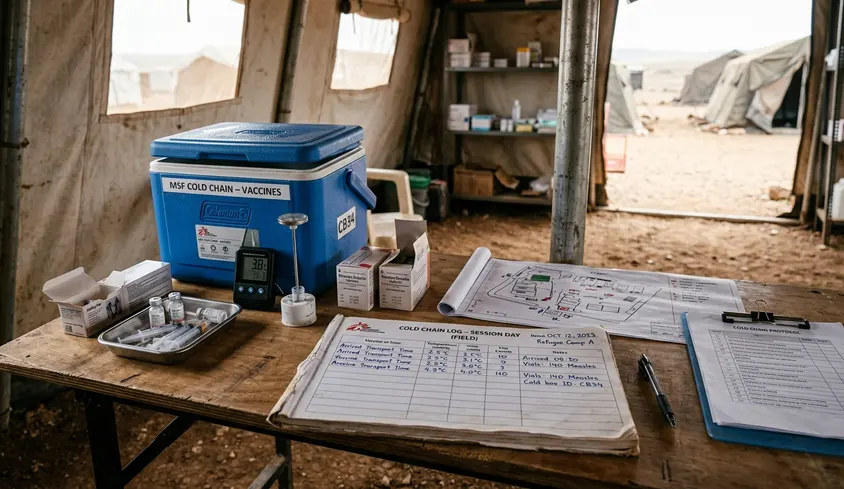
Monitor, Document, and Respond to Temperature Excursions
Temperature monitoring is a decision system, not a paperwork ritual.
A useful log tells the team whether vaccines can continue in use, whether stock must be segregated, and who has authority to release, retain, or discard it. If the log cannot support those decisions, it is decoration.
Public-health responders often use standardized cold chain logs and incident escalation pathways so field teams do not make isolated clinical decisions under pressure. That matters in camp settings, where a mobile team may be working far from the senior clinician, pharmacist, or EPI focal point.
What a temperature record should capture
- Time of the check.
- Location of the vaccine or equipment.
- Equipment identifier for the refrigerator, cold box, or carrier.
- Monitor reading and any visible condition concerns.
- Carrier or refrigerator status, including lid opening, power status, or ice pack condition when relevant.
- Staff initials.
- Action taken.
- Escalation contact or decision authority.
Suspected excursions should trigger immediate segregation and labeling pending review. Staff should not argue over a vial at the table while the queue waits. Move the stock out of circulation, document what happened, notify the designated authority, and continue only with stock that remains within the approved handling pathway.
One constraint: standard escalation pathways often assume that phones work. In camps with frequent cellular blackouts, teams need pre-authorized local quarantine steps so they can hold questionable stock safely until communication returns.
This is also where roles matter. The person who notices a reading may not be the person authorized to release stock. The plan should make that distinction before the campaign begins.
Scope, Limitations, and Coordination Boundaries
This article is an educational planning framework. It is not a substitute for national immunization policy, vaccine package inserts, manufacturer instructions, or incident-specific guidance from health authorities.
WHO guidance, national EPI procedures, and experienced humanitarian logisticians each cover different parts of the problem. WHO materials help structure practical immunization work. National EPI procedures define the authorized rules for the country. Humanitarian logisticians translate those rules into routes, storage layouts, staff tasks, and contingency plans inside the camp.
None of those sources alone replaces field verification. This framework still has to be checked against the exact vaccine, equipment, staffing pattern, and site conditions in front of the team.
The guide also leaves several subjects outside its main scope: pharmacovigilance, clinical eligibility screening, procurement law, campaign ethics, and full biomedical waste management. Those areas need their own technical leads and approvals.
The cold chain succeeds when clinical and logistics teams stop treating it as a back-room function. It is part of the campaign design from the first assumption sheet to the last returned carrier.