In this Article
- What nutrition teams must decide before the first distribution line forms
- Why emergency rations stabilize households but do not treat acute malnutrition
- How screening, triage, and referral catch risk early
- Where outpatient and inpatient therapeutic feeding fit
- How the logistics pipeline protects nutrition outcomes
- Why food, water, disease control, and protection cannot be separated
- How blanket rations and targeted therapeutic feeding work as complementary layers
- Where standards stop and field judgment begins
Key Takeaways: What Nutrition Response Must Decide First
Summary:
- Emergency rations are a population-level logistics intervention. They keep households eating during displacement, supply disruption, or the first weeks of camp establishment.
- Therapeutic feeding is a clinical and public-health pathway for people with acute malnutrition or serious nutritional risk.
- A useful nutrition response depends on screening, referral, steady supplies, safe water, infection control, and caregiver access.
The first mistake in camp nutrition planning is treating food as one problem. It is not.
When a camp opens under pressure, logisticians and medical coordinators need to map two things together: the population’s likely baseline nutritional status and the supply routes that can actually hold up. If the road washes out in three weeks, the ration plan changes. If measles risk is rising in a crowded sector, the therapeutic feeding plan changes too.
General rations answer one question: can households maintain basic food access today and tomorrow? Therapeutic feeding answers another: who is already in danger, and what clinical pathway keeps that person alive long enough to recover?
Those decisions overlap, but they are not interchangeable.
Why Emergency Food Rations Are Not a Complete Nutrition Response
Rations Buy Time
Emergency food rations stabilize households when people have lost farms, wages, markets, kitchens, or all four. A planning target often used for general food aid is around 2,100 kilocalories per person per day, but the number is only the start of the argument. The harder question is whether the ration can be transported, stored, cooked, shared, and safely consumed in the camp that exists, not the camp drawn on the planning map.
I have watched ration design change because the camp had grain mills but not enough cooking fuel. Cereals looked efficient in the warehouse. They looked less efficient when caregivers spent half the afternoon searching for firewood.
Dry rations, cooked meals, fortified blended foods, and cash or voucher support all solve different problems. Dry rations give families control, but they require fuel, water, utensils, and storage space. Cooked meals help during the earliest phase when households have nothing, but queues can become unsafe and the system needs a constant prepared-food operation. Fortified blended foods bring micronutrients into the ration basket. Cash or vouchers can work where markets function and prices stay within reach.
The Practical Tension
Ration planning is full of trade-offs. Calories matter, but so do micronutrients, cultural acceptability, queue safety, packaging strength, cooking time, and the risk of theft inside shelters. A cereal-heavy basket may move well by truck. A food that nobody cooks properly because water is scarce will not do the job.
Quick Tip: Before expanding a ration item, ask four field questions: can people cook it, can they store it, can they carry it, and will they actually eat it?
This is why emergency rations are necessary but incomplete. They reduce household food pressure. They do not diagnose a wasted child, treat edema, manage dehydration, or follow up a pregnant woman who missed the last distribution.
Screening, Triage, and Referral: Finding Nutritional Risk Early
How Teams Find Risk
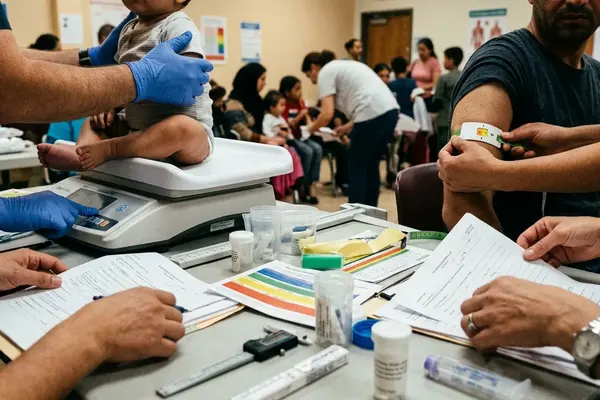
Good screening starts before the clinic fills up. Community health workers move through camp sectors, reception points, transit shelters, and food lines looking for people who will not present themselves unless someone asks. Admission screening catches some cases. Growth monitoring catches others. Caregiver reports often catch the cases that look ordinary from a distance.
In a crowded camp, a color-coded MUAC tape is one of the fastest tools in the room. For children aged 6 to 59 months, a mid-upper arm circumference measurement below 115 mm indicates severe acute malnutrition and requires urgent referral through the nutrition pathway. Edema checks matter just as much. So do appetite assessment, fever history, diarrhea, cough, lethargy, and the caregiver’s account of what changed last week.
These tools classify risk; they do not predict whether a caregiver can return next week through a flooded road or a tense checkpoint.
Triage Cannot Stay in the Nutrition Tent
Nutrition triage has to connect with measles risk, diarrhea, respiratory infection, pregnancy, lactation, disability, and child protection. An unaccompanied child with a borderline screening result may be at higher practical risk than the form suggests. A lactating mother who skipped food distributions because the queue was unsafe may deteriorate quickly even if she looks stable at first contact.
Stakeholder feedback indicates that referral systems fail most often at the handoff: the community worker finds the person, but the clinic queue, registration desk, or caregiver schedule breaks the chain. That is not a medical mystery. It is an access problem.
Therapeutic Feeding Pathways: Outpatient, Inpatient, and Stabilization Care
Three Different Clinical Situations
Therapeutic feeding is not one queue with different products at the end. It sorts people by clinical risk.
- Moderate nutritional vulnerability may need supplementary feeding, counseling, infection checks, and close monitoring.
- Severe acute malnutrition without major complications may be managed through outpatient therapeutic care when appetite is present and follow-up is realistic.
- Severe cases with complications need inpatient stabilization, especially when infection, poor appetite, dehydration risk, or medical instability is present.
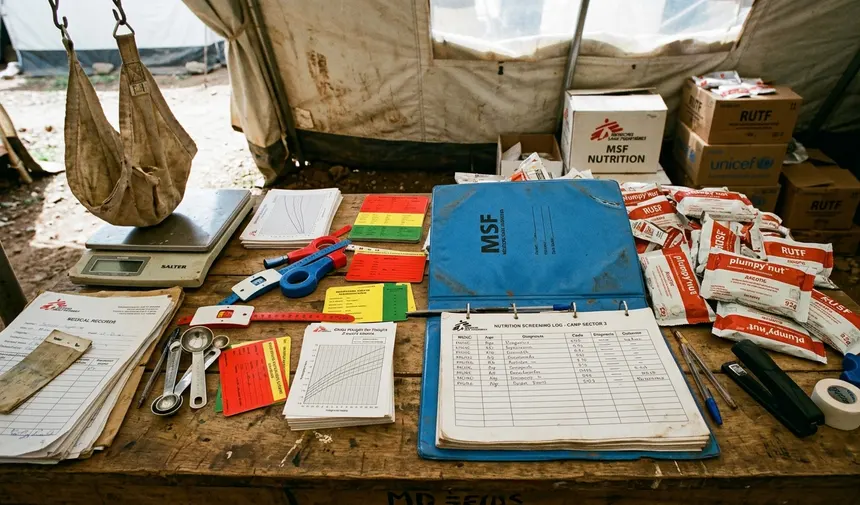
Clinicians commonly use an appetite test with ready-to-use therapeutic food. If the child eats the product and has no severe medical complications, outpatient care may be appropriate. If the child cannot eat, appears medically unstable, or shows signs that need close observation, the pathway shifts toward inpatient stabilization.
Outpatient Care Is Clinical Work, Not Just Product Distribution
Outpatient therapeutic programs depend on ready-to-use therapeutic foods, scheduled follow-up, appetite checks, weight or growth monitoring, and caregiver counseling. A standard outpatient recovery period is often planned around 6 to 8 weeks, though mobility, insecurity, illness, and household pressure can shorten or interrupt treatment.
Caregiver counseling is not decorative. Families need to know that the sachet is medicine-like nutrition for the enrolled person, not a snack for the whole shelter. That message can be hard to honor when siblings are hungry.
For clinical protocols, the WHO guidance on the management of severe acute malnutrition remains a key reference point, adapted through national protocols and field constraints.
Stabilization Care Handles the Fragile Edge
Inpatient stabilization is where nutrition and medicine become inseparable. A severely malnourished child with infection, poor appetite, or dehydration risk cannot simply receive a carton of product and instructions for next week. The team needs observation, careful feeding progression, infection management, and a discharge plan that does not collapse at the camp gate.
Adults may need stabilization too, especially older people, people with chronic illness, and those weakened by long journeys. Camps often miss them because screening systems focus heavily on young children. That focus is understandable, but it leaves blind spots.
The Logistics Pipeline Behind Every Sachet, Sack, and Distribution Line
From Forecast to Follow-Up
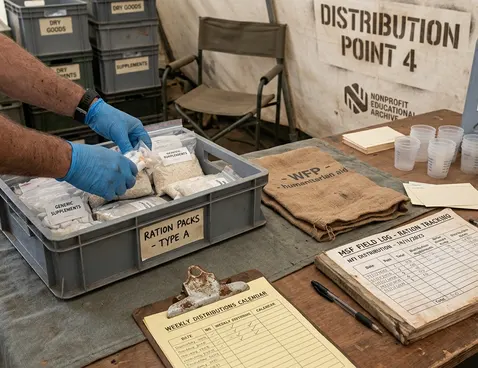
Every sachet of therapeutic food and every sack of grain sits at the end of a long operational chain. Forecasting comes first: expected population size, admission trends, seasonal disease patterns, and likely access constraints. Procurement follows. Then transport, warehousing, ration cards, crowd management, distribution, stock reconciliation, and post-distribution monitoring.
MSF-style field logistics thinking is useful here because it links clinical outcomes to hard operational habits: stock rotation, secure warehousing, vehicle access, fuel planning, cold chain discipline where nutrition products or linked medicines require temperature control, and last-mile delivery that still works after rain turns the road into mud.
Supply chain managers may pre-position buffer stock 3 to 6 months ahead of rainy seasons when roads predictably fail. That is not hoarding. It is the difference between a planned distribution and ration halving after the first bridge washes out.
Where the Pipeline Breaks
Pipeline breaks rarely announce themselves as one dramatic event. They show up as smaller cuts: expired products at the back of the store, damaged packaging, missing waybills, theft risk, fuel shortages, or a truck that cannot pass the last flooded stretch. Then the distribution team starts reducing quantities, delaying rounds, or prioritizing one group over another.
Monitoring reports show that exclusion errors often come from ordinary administrative friction: a lost ration card, a misspelled name, a family newly arrived after registration closed. The food may be in the warehouse and still not reach the household that needs it.
Note: A clean stock ledger does not guarantee a clean nutrition outcome. The ledger can be correct while queues remain unsafe, caregivers miss appointments, or sharing dilutes therapeutic intake.
Food, Water, Disease, and Protection Are Operationally Inseparable
Nutrition Deteriorates Fast in a Dirty Environment
A ration basket cannot compensate for unsafe water, uncontrolled diarrhea, overcrowded shelters, poor sanitation, or missed vaccination opportunities. The minimum survival allocation often cited for emergency water planning is roughly 15 to 20 liters of safe water per person per day. When families fall short, food preparation changes. Handwashing drops. Caregivers stretch water for cooking and cleaning, and children pay the price.
The VIP latrine, the handwashing station, the shaded distribution line, and the disease surveillance register all belong in the nutrition conversation. So does shelter density. A child recovering from acute malnutrition in a damp, crowded shelter with constant respiratory infection risk is not on the same trajectory as a child recovering in a stable household space.
Protection Shapes Access
Site planners who understand distribution lines map the sun, not just the crowd. Shade matters. So do handwashing stations, fast-track lanes for pregnant women and older people, and arrangements for people with disabilities who cannot carry a full ration home.
Women and children often spend the longest time in food queues. If the queue is exposed, tense, or far from shelter, attendance drops. If households lack cooking pots, lids, fuel, or safe storage containers, the ration loses practical value before it reaches the plate.
Food assistance is not only about food.
Field Comparison: Blanket Rations Versus Targeted Therapeutic Feeding
Complementary Layers, Not Competing Systems
Blanket rations and targeted therapeutic feeding answer different questions at the same time. Blanket distributions ask: how do we stabilize the whole population? Therapeutic feeding asks: who needs clinical nutrition support right now?
The two systems work best as layers. Blanket rations reduce the pressure that drives sharing of therapeutic foods. Targeted feeding catches the people who will not recover through general household food access alone.
Operational Comparison: Blanket Rations vs. Targeted Therapeutic Feeding
- Primary objective: Blanket emergency rations support population-level food security and stabilization. Targeted therapeutic feeding treats acute malnutrition and closely related clinical risk.
- Eligibility: Blanket rations usually follow household registration or camp-wide criteria. Therapeutic feeding follows screening, clinical assessment, and referral.
- Product type: Blanket systems may use cereals, pulses, oil, fortified blended foods, cooked meals, cash, or vouchers. Therapeutic programs use specialized products such as ready-to-use therapeutic foods and clinical feeding supplies.
- Distribution frequency: Blanket rations often run on scheduled cycles. Therapeutic feeding requires follow-up visits, appetite checks, and adjustment based on clinical status.
- Monitoring method: Blanket programs rely on distribution records, stock reconciliation, and post-distribution monitoring. Therapeutic programs track admission, progress, default, referral, and recovery status.
- Staff skills: Blanket distributions lean heavily on logistics, registration, crowd management, and accountability. Therapeutic feeding requires nutrition staff, clinicians, community health workers, and referral coordination.
- Main risks: Blanket rations face diversion, exclusion errors, queue safety problems, and pipeline breaks. Therapeutic feeding faces household sharing, loss to follow-up, product acceptability problems, and missed medical complications.
A field coordinator should not have to choose between the two unless supplies or access force a temporary triage decision. In a functioning response, blanket rations lower the background hunger level while therapeutic feeding concentrates clinical attention where the risk is highest.
Scope, Limitations, and What Standards Cannot Solve Alone
Guidance Needs Field Judgment
Standards help teams move quickly, speak a common technical language, and avoid improvising clinical care from scratch. They do not remove judgment. Camp nutrition response varies by emergency phase, population profile, disease burden, access constraints, supply routes, and national protocols.
A protocol written for a stable camp can strain in a mobile border setting. One catch: therapeutic feeding protocols assume a stable household environment; high displacement mobility often results in treatment default before the standard recovery period is reached.
The Limits Are Practical and Human
Rations get shared. Therapeutic foods get shared too, especially when the rest of the household is hungry. Follow-up visits get missed because caregivers are collecting water, searching for fuel, caring for other children, or avoiding unsafe routes. Product acceptability varies. Staff shortages slow screening. Insecurity closes roads. Market disruption can make cash assistance unreliable almost overnight.
Data gaps also matter. Admission numbers may rise because malnutrition worsened, because outreach improved, or because a nearby clinic closed and sent everyone to the camp. Program evaluation revealed lessons only when nutrition, logistics, water, health, and protection teams compared notes rather than defending their own dashboards.
Summary: A camp nutrition response works when general rations, therapeutic feeding, water systems, disease control, and protection planning reinforce one another. Separate them on paper if you must. In the field, they arrive at the same household.