
Key Takeaways for Intake Teams
Summary: A workable malnutrition screening pathway starts with rapid MUAC triage at the entry point, sends indicated children to weighing and measuring, then routes them into supplementary or therapeutic care. MUAC gets the line moving. Weight-for-height with Z-Scores gives a more detailed anthropometric assessment when equipment, time, and trained staff are in place.
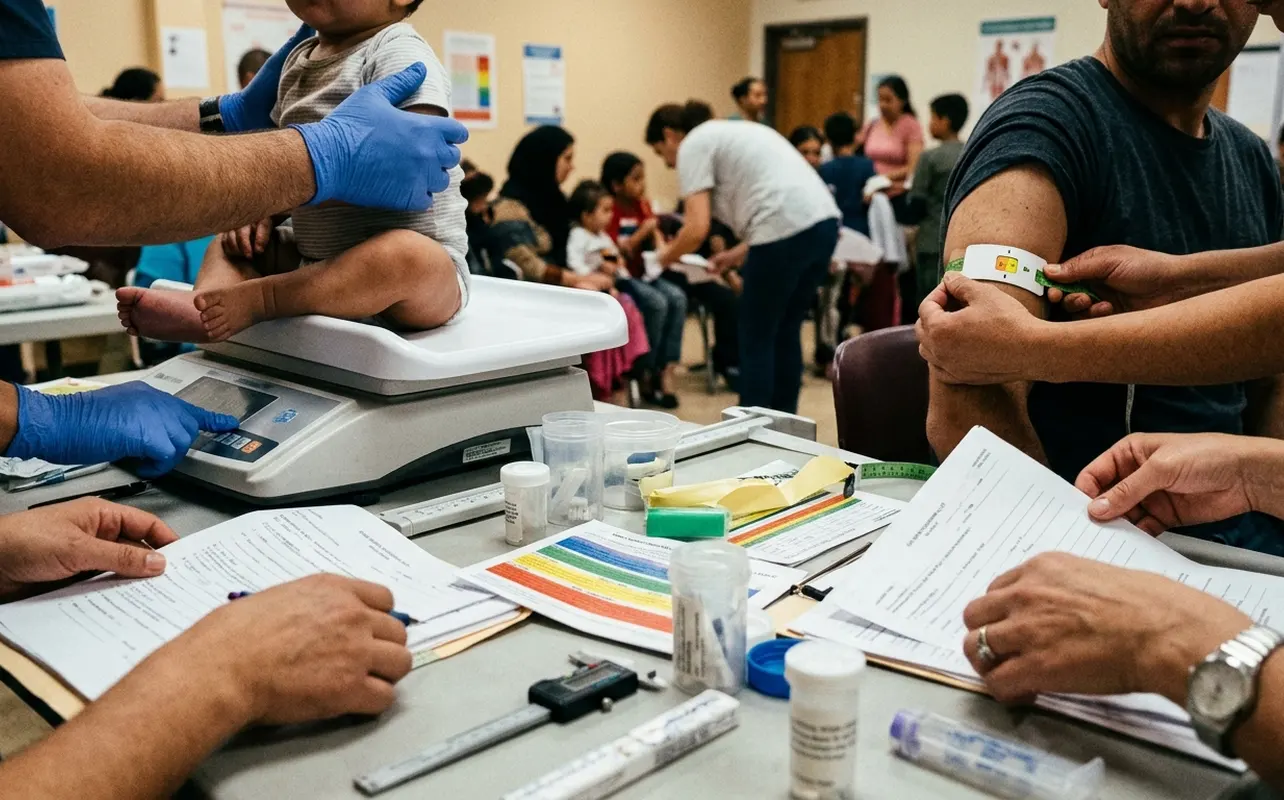
In a crowded reception area, the first job is not to complete every measurement on every child. The first job is to find the child who cannot wait.
- Red MUAC band: severe acute malnutrition and urgent movement toward therapeutic care.
- Orange MUAC band: moderate acute malnutrition and routing toward supplementary feeding.
- Yellow MUAC band: mandatory referral to weighing and measuring stations for further assessment.
That color logic is useful because it is simple, visible, and fast. It is also easy to misuse if the team treats the armband as the whole diagnosis. MUAC is an entry screen; weight-for-height using Z-Scores adds a more detailed assessment when the site has stable scales, measuring equipment, and staff who know how to use them consistently.
The practical sequence is straightforward: rapid screen, document the color band, send the child to the right next station, and make sure the referral does not disappear between tents.
The Arrival Flow: From Queue to Referral Decision
I have watched intake points slow down when the weighing station sits too close to registration. Families bunch around the scale, screeners lose the order of arrival, and the child who looks weakest can end up waiting behind paperwork.
A better layout physically separates the quick decision from the detailed assessment. Families enter through the registration queue, move into a shaded waiting area, pass a first-look clinical observation point, then reach the MUAC station. Only children who need it move onward to weighing and measuring. The last stop is a referral desk, where the intake slip tells the caregiver where to go next.
What the layout looks like on the ground
In a refugee camp, this is rarely a neat diagram on a clipboard. The reception area may sit beside shelters covered in UNHCR blue plastic sheeting. Shade may come from payottes, the traditional shaded meeting places that families already recognize as places to gather. Water bladders may sit near the registration queue because basic services have to be close enough for newly arrived families to use them without losing their place.
That ground reality matters. A shaded line is not a comfort feature; it keeps children from deteriorating while they wait. Clean water beside the queue helps caregivers, staff, and children get through the intake process without turning screening into another stressor.
Who moves first
Every child should pass through a standardized pathway, but not every child should wait at the same pace. Screeners need authority to move visibly wasted, lethargic, edematous, febrile, dehydrated, or unable-to-feed children forward for immediate clinical review.
Note: Priority movement should not become informal guessing. The same intake slip still travels with the child, and the same destination decision still has to be documented.
MUAC Triage: Reading the Armband Without Overreading It
MUAC means Mid-Upper Arm Circumference. The measurement is taken with a MUAC armband around the child’s upper arm to identify children who need nutrition attention quickly.
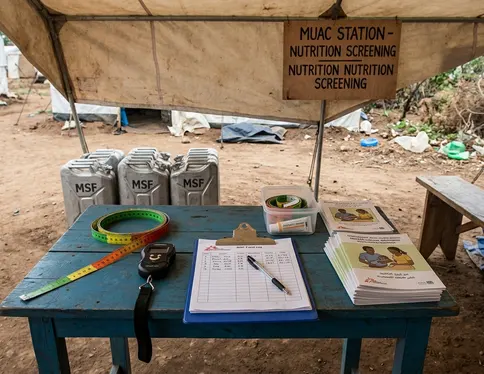
The technique is simple enough to teach under pressure, but it is not casual. Screeners locate the midpoint of the upper arm, place the tape flat against the skin, and avoid pulling so tightly that soft tissue is compressed. A rushed hand can change the reading. A twisted tape can send a child to the wrong station.
The color bands carry the pathway logic:
- Red indicates severe acute malnutrition.
- Orange indicates moderate acute malnutrition.
- Yellow triggers referral to weighing and measuring.
Immediate documentation matters as much as the reading itself. The color band and referral action should be written on the patient intake slip before the caregiver leaves the station.
The armband is a trigger, not the whole case
MUAC should not be treated as a full diagnosis in isolation. Measurement quality, the child’s age group, edema assessment, danger signs, and the current local protocol all affect the final decision.
Quick Tip: If the MUAC station is producing many unclear readings, do not blame the armbands first. Watch the hands. Tape tension, arm position, and staff fatigue often explain the problem.
Weight-for-Height and Z-Scores After the First Screen
Weight-for-height, often written as W/H, is the next layer of anthropometric assessment when a child needs more detail after initial triage. It compares the child’s weight with height or length and uses Z-Scores in standard W/H tables.
A Z-Score is a statistical measure used in those tables. This article does not assign numeric cutoff values because the supplied context does not provide source-verified thresholds. That restraint is deliberate. In nutrition screening, a confident number without the right source can cause more harm than a cautious explanation.
Equipment makes or breaks the assessment
Salter scales in 25kg and 50kg capacities are part of standard weighing setups. They need routine calibration, stable hanging points, and staff who understand how wet clothing can distort the measurement. If a caregiver has just crossed rain or floodwater, the weighing station should not pretend those clothes are invisible.
Measuring boards or height methods also need consistency. Young children must be positioned fully and calmly. The board should not wobble. The measurer should not improvise a new technique each time the queue grows.
Program evaluation revealed the same operational lesson in different emergencies: the detailed assessment only helps when the measurement environment is controlled enough to trust the result.
Routing Children to SFP, TFP, or a Therapeutic Feeding Center
The routing decision turns screening into care. Moderately malnourished children move toward SFP, the Supplementary Feeding Program. Severely malnourished children move toward TFP, the Therapeutic Feeding Program. Children with severe or clinically complicated cases may require admission to a TFC, the Therapeutic Feeding Center.
Dry and wet supplementary feeding are not the same operation
An SFC dry model sends supplementary rations home with the caregiver. That can reduce crowding at the feeding site and may fit families who can prepare food safely. An SFC wet model provides meals consumed on-site, which gives teams more direct control over preparation and consumption but requires more space, water, staff time, and queue management.
The right model depends on what the camp can support that week, not just what the protocol prefers on paper. Food commodities are tied to distribution cycles, and WFP’s role is most visible when the pipeline affects what a feeding program can actually provide. In some emergency settings, food distribution cycles occur roughly every two weeks, which forces program managers to think hard about ration timing and caregiver instructions.
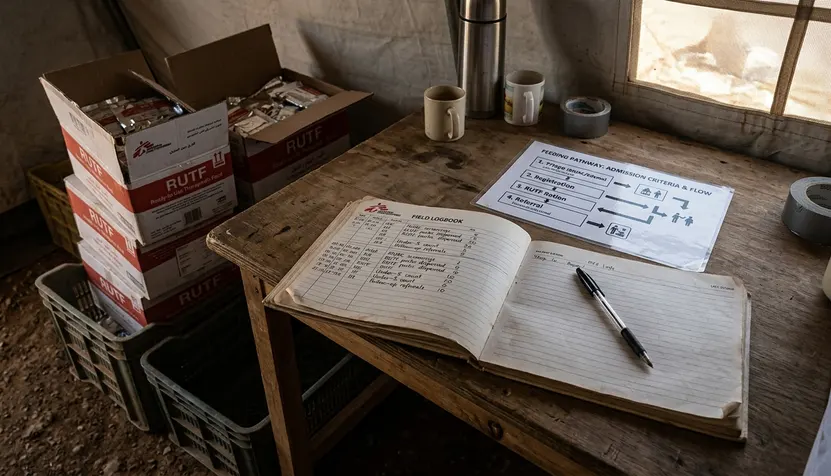
When therapeutic feeding becomes clinical care
Therapeutic Feeding Centers require closer observation than a routine distribution point. Staff monitor feeding capacity, danger signs, hydration concerns, and whether the child can take nutrition safely by mouth.
Specialized supplies may be needed. CH No. 8 and No. 10 Luer naso-gastric tubes are used when therapeutic feeding support is medically indicated. That detail belongs in logistics planning, not as an afterthought once the child is already admitted.
Summary: Screening does not end with the color band. The pathway must land the child in a real program: SFP for moderate cases, TFP for severe cases, and TFC admission when severity or clinical complications require closer care.
Logistics That Determine Whether Screening Works
Nutrition screening depends on clinical knowledge, but it survives on logistics. Shade, queue control, clean water, scales, MUAC armbands, forms, referral slips, feeding supplies, and enough staff to keep each station from collapsing into the next one: these are not background items.
MSF designs standardized nutrition kits for emergency response, helping teams deploy repeatable screening and feeding workflows quickly. In practice, that means the MUAC tapes, scales, paperwork, and therapeutic supplies are planned as a package rather than chased one by one after arrival numbers climb. MSF-USA may support project administration where that role fits the operation, but the field value is concrete: the right materials arrive in a form teams can use.
UNHCR’s blue plastic sheeting matters differently. It is not a nutrition tool, but it shapes the reception environment where screening happens. A shaded shelter line can keep the intake pathway safer. A VIP latrine nearby can protect dignity and reduce avoidable contamination around a feeding site.
Transport is part of the protocol
Flood plains that remain underwater for several months of the year can disrupt transport of standardized emergency nutrition kits. That is not a side problem for the logistics team; it can decide whether the screening protocol exists beyond the first page.
Grant data supports the plain operational point: supplies, staffing, and site access need to be planned together. A camp can have trained screeners and still fail to screen well if the armbands are in a warehouse across a flooded road.
Why Nutrition Screening Must Sit Beside Outbreak Control
The 1992 measles epidemic context is a hard reminder that nutrition teams and public health teams cannot run parallel emergencies as if they do not touch. Viral threats can rapidly deplete nutritional reserves in displaced children. Malnutrition then complicates clinical risk, feeding capacity, recovery, and follow-up.
In the Bassikounou camp context in Mauritania, affected populations included Tuaregs, Malian Moors, and non-immunized nomadic families. A May 1992 epidemiological investigation, with Epicenter as the research and epidemiology partner, placed the nutrition question inside a wider outbreak-control problem rather than treating it as a separate service line.
That history matters because intake teams often see the child before the disease-control system has finished mapping the outbreak. A child who is febrile, dehydrated, unable to feed, or visibly wasted cannot be routed by nutrition status alone. The referral desk must know how to move the child into clinical review, immunization follow-up, isolation procedures when relevant, or feeding support without making the caregiver navigate separate queues.
For broader clinical orientation after resettlement, the CDC domestic guidance on nutrition and growth is useful, though camp intake decisions still depend on the responsible health authority and the emergency protocol in force.
Scope, Limitations, and Minimum Documentation
This article is an educational pathway for understanding camp intake screening. It is not a substitute for the current clinical protocol of the responsible health authority.
It also avoids numeric MUAC or W/H thresholds because the supplied context does not provide source-verified cutoff values. That is not a missing detail to patch with memory. Cutoffs must come from the active protocol, the age group being screened, and the health authority responsible for the program.
Historical examples from Mauritania, Somalia, and Eastern Thailand help explain operational problems, but each emergency still requires localized assessment rather than rigid reuse of past protocols.
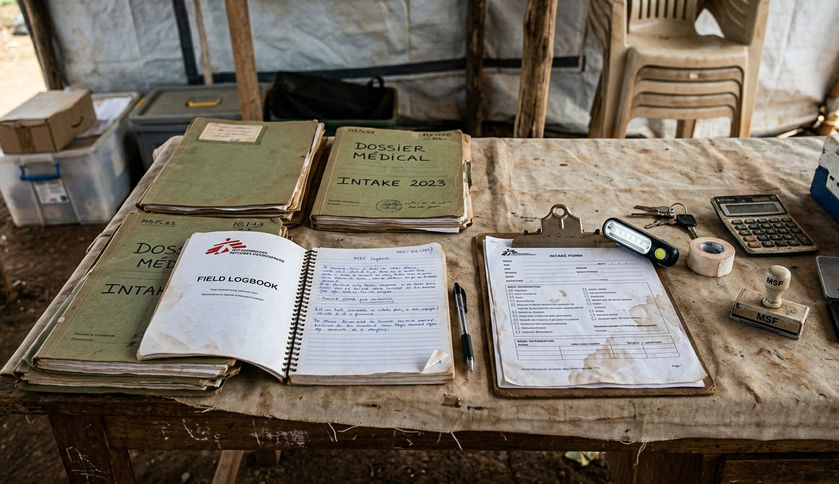
Minimum documentation fields
At intake, the documentation should be simple enough to complete under pressure and specific enough to trace the child’s movement through the system. Minimum fields include:
- Child identifier.
- Age category, if known.
- MUAC color band.
- W/H referral status.
- Edema or danger-sign note.
- Destination program.
- Follow-up instruction.
The form does not need to be elegant. It needs to travel with the child, survive the handoff, and make the next decision easier.
That said, a screening pathway is only as strong as its weakest handoff. If the MUAC station, weighing station, and referral desk do not share the same documentation logic, children can be correctly identified and still fail to reach care.







